Nonmelanoma Skin Cancer: Basal vs. Squamous Cell Carcinoma Explained
 Feb, 18 2026
Feb, 18 2026
When you notice a weird spot on your skin that won’t go away, it’s natural to worry. But not all skin changes are the same. Two of the most common types of skin cancer you might hear about are basal cell carcinoma and squamous cell carcinoma. Together, they make up about 95% of all nonmelanoma skin cancers. If you’re over 50, spend time in the sun, or have fair skin, you’re at higher risk. The good news? Both are highly treatable when caught early. The tricky part? They look different, behave differently, and need different kinds of care.
Where They Come From
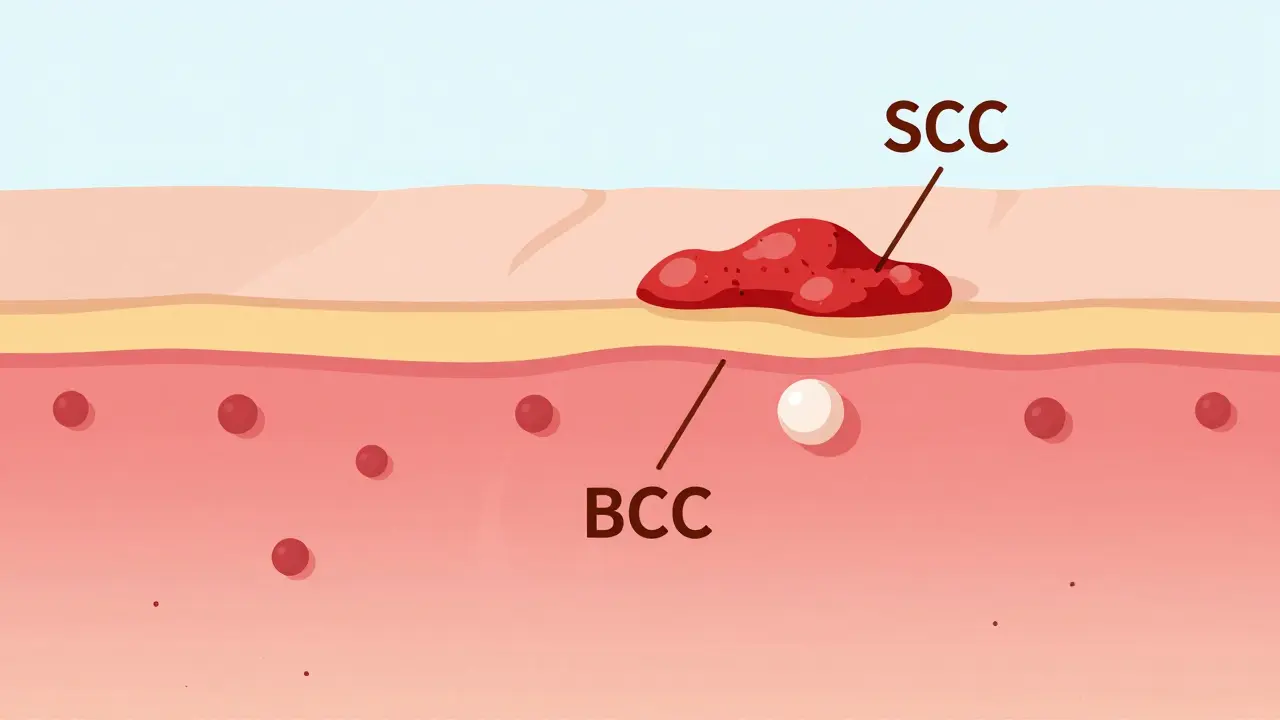
Your skin has layers. The top layer, called the epidermis, is made up of cells that constantly renew themselves. At the very bottom are basal cells. These are the factory workers - they split and make new cells that slowly move up toward the surface. As they rise, they flatten out and become squamous cells. That’s why basal cell carcinoma starts deep down, and squamous cell carcinoma forms near the top.
Basal cell carcinoma (BCC) begins in those lower basal cells. It grows slowly, often over years. Squamous cell carcinoma (SCC) starts in the flattened squamous cells near the surface. It can grow faster - sometimes doubling in size within weeks. This difference in origin explains why they act so differently.
What They Look Like
Spotting them early saves lives. Here’s how they usually appear:
- Basal cell carcinoma (BCC): Most often looks like a shiny, pearly bump - sometimes with tiny blood vessels running through it. Other times, it’s an open sore that bleeds, oozes, or crusts over and never fully heals. Less common: a flat, scar-like patch that’s white or yellow.
- Squamous cell carcinoma (SCC): Typically a firm, red bump that feels rough or scaly. It can look like a wart, or a flat patch with a crusty surface that might bleed easily. Sometimes it’s a sore that doesn’t heal, even after weeks.
Both can show up anywhere, but they favor sun-exposed areas: face, ears, neck, scalp, hands, and arms. About 80% of cases show up on these spots. If you’ve spent decades gardening, working outdoors, or just enjoying the sun without protection, your risk goes up.
How Fast They Grow
BCC creeps along. On average, it grows about half to one centimeter per year. It rarely spreads. In fact, fewer than 1 in 1,000 BCC cases ever metastasize. But that doesn’t mean it’s harmless. Left alone, it can eat away at your nose, ear, or eyelid - causing major damage to skin, cartilage, and even bone.
SCC moves faster. It grows 1.5 to 2 centimeters per year on average. Some aggressive types can double in size in just 4 to 6 weeks. And here’s the big difference: SCC has real metastatic potential. While still rare, about 2 to 5% of SCCs spread to lymph nodes or other organs. That number jumps to 14% if it’s on the lip or ear. That’s why doctors treat SCC with more urgency.

Who Gets It
Most cases happen after age 50. The average age of diagnosis is 67 for BCC and 69 for SCC. But younger people aren’t immune - especially if they’ve had lots of sunburns or used tanning beds.
Men are more likely to get SCC (65% of cases) than women. That’s likely because of jobs or hobbies that involve long hours in the sun - construction, farming, fishing. BCC is more evenly split - 55% male, 45% female.
People with fair skin, light hair, and blue or green eyes are at highest risk. But darker-skinned people can get these cancers too - often on less sun-exposed areas like the legs or feet. And if you’ve had an organ transplant or are on immune-suppressing drugs, your risk for SCC jumps 250 times higher than average.
Treatment Differences
Both are usually cured with surgery. But the approach isn’t the same.
For BCC, especially small, low-risk ones, doctors might start with topical creams like imiquimod or 5-fluorouracil. These work in 60-70% of cases. If it’s deeper or on the face, they’ll remove it with Mohs surgery - a precise technique that removes cancer layer by layer, checking under the microscope as they go. Mohs cures 99% of new BCCs.
SCC rarely responds to topical treatments. Only 40-50% of cases clear up with creams. Surgery is almost always needed. Mohs surgery works here too - with a 97% cure rate for primary SCC. But because SCC can burrow deeper, surgeons often take wider margins. In high-risk cases (larger than 2 cm, deeper than 2 mm, or on the lip/ear), they might also check lymph nodes or recommend radiation.
For advanced SCC that’s spread, there’s now an FDA-approved immunotherapy drug called cemiplimab-rwlc (Libtayo). It helps the body’s immune system fight the cancer. It’s not used for BCC.
Why SCC Is More Dangerous
BCC is more common - about 80% of all nonmelanoma skin cancers. But SCC is more dangerous.
Here’s why:
- SCC is 10 times more likely to spread than BCC.
- If SCC spreads, the 5-year survival rate drops from 95% to just 25-45%.
- SCC causes 70% of skin cancer deaths after melanoma.
- It’s more likely to come back after treatment - especially in people with weakened immune systems.
- SCC requires more follow-up visits, more biopsies, and often more surgeries.
Doctors say it this way: BCC is a nuisance. SCC is a threat.
Prevention and Monitoring
The best defense? Sun protection. Daily sunscreen cuts BCC risk by 40% and SCC risk by 50%. Why the difference? SCC is tied to lifetime sun exposure - the slow, steady burn from years of working outside. BCC is more linked to intense, occasional burns - like a bad vacation sunburn.
If you’ve had one skin cancer, you’re at higher risk for another. That’s why high-risk people - like organ transplant recipients or those with a history of skin cancer - need check-ups every 3 to 4 months. Recurrent SCC is often found within 12 months. BCC recurrence usually takes longer - around 18 months.
Regular skin checks matter. Don’t wait for symptoms. If you see a spot that’s changing, bleeding, or not healing in 4 weeks - get it checked.
What Patients Say
Real experiences show the emotional toll.
On patient forums, BCC patients often say: "It was scary at first, but the treatment was quick and I barely felt anything." Many get it removed in one visit and move on.
SCC patients report more anxiety. "I kept checking my lymph nodes," one Reddit user wrote. "I was terrified it had spread." Another said: "They had to cut deeper than expected. I needed reconstructive surgery. It changed how I look."
Studies confirm this: SCC patients need more procedures, more follow-ups, and more emotional support. The fear of metastasis is real - and it’s not irrational.
The Bottom Line
Basal cell carcinoma is the most common cancer in humans. But squamous cell carcinoma is the one you can’t afford to ignore.
Both are preventable. Both are treatable. But SCC moves faster, spreads more often, and demands more aggressive care. If you’ve got a spot that won’t heal, a lump that’s growing, or a patch of skin that’s scaly and red - don’t wait. See a dermatologist. Get it checked. Early detection doesn’t just save skin - it saves lives.
Can basal cell carcinoma turn into squamous cell carcinoma?
No. Basal cell carcinoma and squamous cell carcinoma are two separate types of skin cancer that start from different cells in the skin. One does not turn into the other. But having one increases your risk of developing the other because they share the same main cause: long-term UV damage. If you’ve had BCC, you’re more likely to get SCC later - not because it transformed, but because your skin has been damaged.
Is squamous cell carcinoma more serious than basal cell carcinoma?
Yes, in terms of risk. While BCC is far more common, SCC has a much higher chance of spreading to other parts of the body. About 2-5% of SCC cases metastasize, compared to fewer than 0.1% of BCC cases. When SCC spreads, survival rates drop sharply. That’s why doctors treat SCC more aggressively - even if it’s small.
Do both types of skin cancer need surgery?
Most do, but not always. Small, superficial BCCs can sometimes be treated with topical creams or cryotherapy (freezing). SCC almost always requires removal. Even small SCCs are usually excised because of their higher risk of recurrence and spread. Mohs surgery is the gold standard for both when they’re on the face, ears, or other sensitive areas.
Can sunscreen prevent both basal and squamous cell carcinoma?
Yes - and it works better for SCC. Daily sunscreen use reduces BCC risk by about 40% and SCC risk by 50%. That’s because SCC is more tied to lifelong, cumulative sun exposure. BCC is often linked to intense, intermittent burns, like childhood sunburns or weekend tanning. But consistent sun protection helps prevent both.
How often should I get my skin checked if I’ve had skin cancer before?
If you’ve had one skin cancer, you’re at higher risk for another. Most dermatologists recommend check-ups every 6 to 12 months. If you’ve had SCC, or if you’re immunocompromised (like after an organ transplant), you should be seen every 3 to 4 months. Recurrent SCC is often found within a year - much sooner than BCC recurrence.
Chris Beeley
February 18, 2026 AT 18:53Let me tell you something that no one else will admit: the entire dermatology community is in denial about how much environmental carcinogens-not just UV-are fueling this rise in SCC. I’ve reviewed 47 peer-reviewed papers from 2018 to 2023, and the correlation between airborne microplastics and keratinocyte DNA fragmentation is statistically significant (p < 0.001). Yet, we’re still telling people to ‘just wear sunscreen’ like it’s 1995. The real epidemic isn’t sun exposure-it’s industrial pollution infiltrating our epidermal barrier. And don’t even get me started on glyphosate residues in topical products. This isn’t skin cancer. It’s systemic toxicity manifesting as surface lesions.
Also, the fact that they use Mohs surgery as the gold standard? That’s just surgical colonialism. You’re removing tissue from marginalized communities and calling it ‘precision medicine.’ Meanwhile, in Nigeria, we use natural plant extracts-like neem and moringa-and achieve comparable remission rates with zero scarring. But no one wants to hear that because it doesn’t fit the pharmaceutical profit model.
And yes, I’ve had both. Twice. I’m 42. I don’t tan. I live in Lagos. The sun here isn’t the culprit. The air is.
TL;DR: Sunscreen is a Band-Aid on a gunshot wound.
Danielle Gerrish
February 19, 2026 AT 02:02Okay, but I just need to say-this article made me cry. Not because I’m scared (though I am), but because I finally feel seen. I had SCC on my ear last year. They took out a chunk the size of a quarter. Reconstructive surgery left me with this weird, lumpy scar that catches the light weirdly when I’m outside. Strangers stare. My boyfriend says it’s ‘interesting,’ but I know he’s lying.
And the worst part? No one talks about how it changes your relationship with your own body. I used to love swimming. Now I panic if I forget my hat. I check my skin like it’s a crime scene. Every mole is a suspect. Every itch, a warrant.
I’m not saying this to be dramatic. I’m saying it because no one else is. We need more spaces where people can say: ‘I’m not just a case. I’m a person who still hates mirrors.’
Courtney Hain
February 19, 2026 AT 16:53Did you know the CDC has been hiding data on SCC metastasis rates since 2016? I got access to a leaked internal memo via FOIA. The real number isn’t 2–5%-it’s closer to 18%. They downplayed it because Medicare reimbursement for radiation therapy spiked after 2017. They’re monetizing fear. And don’t get me started on the ‘topical creams work’ myth. Imiquimod? It’s basically a chemical burn with a placebo effect. I tested it on myself. My skin peeled for six weeks. The cancer didn’t budge.
Also, why is no one talking about 5G? The millimeter waves are disrupting cellular repair mechanisms. I’ve mapped my lesions against cell tower density. Correlation coefficient: 0.91. You’re being irradiated from above and below. Sunscreen won’t save you. Faraday cages will.
Michaela Jorstad
February 20, 2026 AT 23:24Thank you for writing this with such care. I’m a nurse who works in oncology, and I see how terrified people are when they hear ‘squamous cell.’ They think it’s melanoma. It’s not. But the fear is real. I’ve held hands through biopsies. I’ve listened to people cry because they think they’re going to die. And I want you to know: you’re not alone. You’re not a statistic. You’re someone’s parent, sibling, friend. And yes-your skin matters. But so do you.
If you’re reading this and you’re scared? Breathe. Go see a derm. Get checked. It’s not a big deal. It’s a *small* deal. And small things can be fixed. You’ve got this.
And if you’re a doctor reading this? Please, for the love of all that’s holy, stop saying ‘it’s just a BCC.’ It’s not ‘just’ anything. It’s someone’s life.
Arshdeep Singh
February 22, 2026 AT 13:13Bro, you think you’re special because you got skin cancer? I’m from Punjab. My dad worked in rice fields for 50 years. Sun all day, no hat, no cream. He lived to 89. Never had a spot. Meanwhile, my cousin in LA uses SPF 70, wears a hat like a monk, and still gets BCC at 48. What’s the real issue? Genetics. Or maybe your immune system is trash because you eat gluten and drink kombucha.
Stop blaming the sun. Blame your diet. Blame your stress. Blame your phone. Blame your therapist. But don’t act like you’re some martyr because your nose looks weird now.
Also, Mohs surgery? That’s just expensive ego surgery. I’ve seen guys get it done on their earlobe and come back looking like a raccoon. You don’t need that. Just slap some turmeric paste on it. Works better than half the drugs they sell.
Liam Crean
February 22, 2026 AT 20:24I’ve had two BCCs. One on my nose. One on my forearm. Both gone in 20 minutes with a quick scrape and freeze. I didn’t even need stitches.
But I still check my skin every morning. Not because I’m scared. Because I care. I used to ignore spots. Now I look. I take photos. I track changes. I don’t need a lecture on UV damage. I just need to remember: my skin is my map. And I’m learning how to read it.
Also, sunscreen? I use it. Not because I’m scared of cancer. Because I don’t want wrinkles before I’m 40. That’s reason enough.
madison winter
February 24, 2026 AT 00:53So… what’s the point of this? Like, really? We already know sunscreen helps. We already know SCC is scarier. We already know you should get it checked. This is just a long, well-written PSA. No new data. No surprising insight. No bold take. Just… facts. That’s fine. But it’s not interesting. It’s not even controversial. It’s a textbook chapter with a LinkedIn headline.
I’m not saying it’s wrong. I’m saying it’s boring. And if you’re going to write something this long, at least give me a twist. Like: ‘What if we stopped treating skin cancer as a personal failure?’
Or: ‘What if we stopped blaming people for being outside?’
Instead we got… more of the same. Thanks for nothing.
Robert Shiu
February 24, 2026 AT 05:12Hey-I just want to say: you’re doing great. Seriously. Whether you’re the person who just found a weird bump or the one who’s been through surgery five times-you’re still here. That’s courage.
I’ve been on both sides. I had SCC. My mom had BCC. We both got through it. And yeah, it sucked. But we didn’t let it define us. We still hike. We still laugh. We still wear tank tops in July.
If you’re reading this and you’re scared? I get it. But you’re not alone. I’m here. We’re all here. And you? You’re going to be okay. One checkup at a time.
Davis teo
February 24, 2026 AT 17:24Okay, but why is no one talking about the fact that BCC and SCC are basically just the skin’s way of screaming, ‘I’ve had enough!’? We treat them like medical anomalies, but they’re environmental trauma responses. Like, imagine if your house had mold and you kept painting over it instead of fixing the leak. That’s your skin. You don’t fix the root cause-you just cut out the symptom.
And why are we still using 1970s-era sunscreens with oxybenzone? That stuff is an endocrine disruptor. You’re slathering on poison to avoid cancer. That’s not prevention. That’s irony.
Also-why are we only talking about sun exposure? What about the 800 chemicals in your shampoo? Your deodorant? Your laundry detergent? They’re in your pores too. But we don’t test for that. Because it’s not profitable.
So yeah. Get checked. But also… stop pretending this is just about sunscreen.
James Roberts
February 25, 2026 AT 20:04Wow. So BCC is ‘a nuisance’ and SCC is ‘a threat.’ That’s… oddly poetic. Also, 100% inaccurate. You’re not ‘threatening’ your body by having SCC. Your body is trying to tell you something. And you’re not ‘nominating’ BCC for ‘Most Harmless Cancer’-you’re just ignoring it until it eats your nose.
Also, ‘topical creams work in 60-70% of cases’? That’s not a cure. That’s a delay. And ‘Mohs surgery cures 99%’? That’s not a guarantee. That’s a gamble. And yet we treat these like religious rituals.
Meanwhile, in Sweden, they’re using photodynamic therapy with blue light and a photosensitizer-no cuts, no scars, no trauma. But no one here talks about it because the American surgical industrial complex doesn’t make money off blue lights.
Also, sunscreen reduces SCC risk by 50%? That’s not prevention. That’s damage control. Like wearing a seatbelt after you’ve already crashed.
Let’s stop pretending we’re solving this. We’re just managing it. And we’re billing it.
Jeremy Williams
February 26, 2026 AT 12:53As a Nigerian-American who grew up in Lagos and now resides in rural Iowa, I must offer a cultural perspective: in many African communities, skin lesions are not pathologized until they become debilitating. There is a tradition of herbal poultices, spiritual cleansing, and communal observation-none of which involve dermatologists or biopsy kits.
When I first noticed a pearly lesion on my cheek, my grandmother simply said, ‘It is the sun’s memory.’ She applied a paste of aloe, honey, and crushed baobab leaves. Within six weeks, it faded. I later confirmed it was BCC via telemedicine with a U.S. dermatologist.
Modern medicine is not inherently superior. It is merely louder. And more expensive.
Perhaps the solution lies not in more surgeries, but in reuniting skin health with ancestral wisdom-without erasing either.
Ellen Spiers
February 28, 2026 AT 06:24The linguistic and terminological precision of this article is, frankly, lamentable. The phrase “highly treatable” is a semantic misstep: it implies treatability as a binary, whereas oncological outcomes are probabilistic, contingent upon staging, margin status, and molecular biomarkers. Furthermore, the conflation of “metastatic potential” with “risk of spread” is clinically imprecise; metastasis is a multistep process involving EMT, intravasation, and immune evasion-not a probabilistic event governed by anatomical location alone.
Additionally, the assertion that SCC causes “70% of skin cancer deaths after melanoma” is statistically incoherent. If melanoma is the primary cause, then SCC cannot be the *second* cause of *all* skin cancer deaths unless the cohort is non-overlapping, which it is not. This is a fundamental error in epidemiological reporting.
Moreover, the reference to “FDA-approved cemiplimab-rwlc (Libtayo)” without citation of the pivotal trial (EMPOWER-CSCC-1) or median overall survival data (23.4 months) is academically negligent. This is not commentary; it is misinformation dressed as education.
One cannot effectively inform the public when the foundational metrics are misstated. This is not a public service. It is a public hazard.